Vision Plans
The Vision Care Plan is designed to encourage you to maintain your vision through regular exams and to help with expenses for prescription glasses and contact lenses. Your Vision Care Plan is administered by EyeMed. With this voluntary plan, you may use in or out-of-network providers, but the level of benefit is higher when you receive care from a network provider. A listing of network providers can be found at eyemed.com or by calling EyeMed directly at 844‑409‑3401.
Once your benefit is effective, visit eyemed.com for details.
For more information, including plan limitations, exclusions, and discounted services; please refer to the Vision Care Summary of Benefits by visiting AskPhin.com. Your provider will verify eligibility of benefits. Visit eyemed.com for details.
EyeMed Vision Basics — Lens Types & Options
EyeMed Vision Basics — A Routine Eye Exam
ECU Health Vision Plan
| EyeMed Benefit Coverage | In-Network | Out-of-Network |
|---|---|---|
Well Vision Exam
|
$20 copay | Covered up to $44 retail |
Frames
|
Included in Prescription Glasses
|
Covered up to $77 retail |
Lenses
|
$20 copay | Covered up to $64 retail* |
| Lens Option | Scratch Coat: $13 copay | Ultraviolet coat $15 copay Tints, solid, or gradients: $15 copay | Anti-reflective coat: $45 copay Polycarbonate: $40 copay | High index 1.6: $55 copay Photochromic: $75 copay |
|
Contacts (instead of lenses)
|
Fit & Follow Up
Contact Lenses
|
Fit & Follow Up
Contact Lenses
|
| Extra Savings and Discounts |
|
- * Single covered up to $34 retail; bifocal covered up to $48 retail; trifocal covered up to $84 retail.
2024 Premiums
Full-Time and Part-Time Team Members—Bi-Weekly Deductions
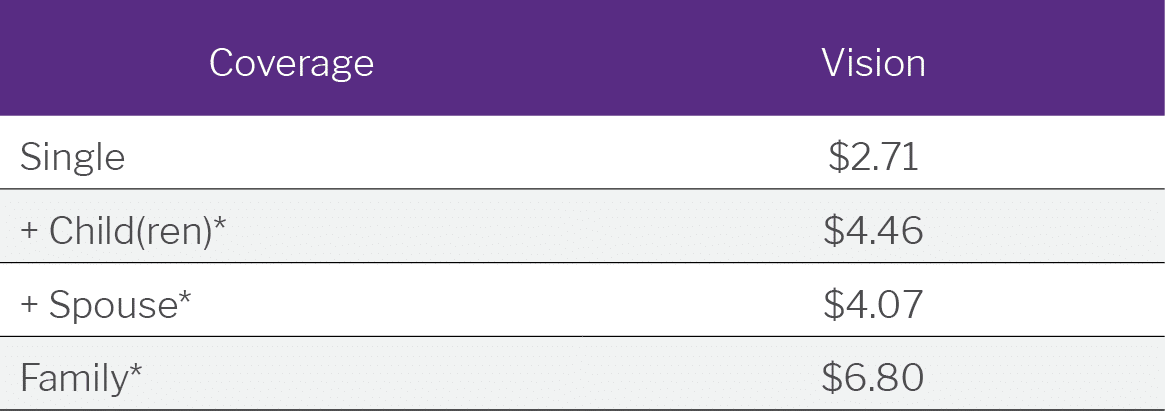
* Includes domestic partner/domestic partner’s children. Family must include you, your spouse/domestic partner and at least one child.